
MY EXPERIENCE AND IMPLICATIONS FOR IMPROVING OUR UNDERSTANDING AND TREATMENT OF HYPERACUSIS
Note: While Hyperacusis Research has seen a number of positive stories on this approach for hyperacusis, we are not aware of any clinical trials for Low-Level Laser Therapy (LLLT). We will continue to follow the research and publish any new clinical findings.[i]
Like most people with hyperacusis, my journey has been long and complex, with many promising leads, apparent dead ends, disappointments—but also discoveries and meetings with amazing people—and a lot of, I am told, personal growth.
I would like to briefly summarize my journey and then focus on my personal experience with low-level laser therapy (LLLT) and some implications for improving our understanding of hyperacusis diagnosis and treatment. I have no investment in claiming LLLT is “effective” or that that it will help others—that’s for good science to find out. As a result of my experience, I propose to broaden our metrics for monitoring the impact of treatment beyond Loudness Discomfort Levels (LDL).
I happened to have an audiogram in early January 2008 following several months of tinnitus. Some of the tones were very uncomfortable, but the tester didn’t mention the possibility of having hyperacusis or even that my response was unusual. Perhaps they didn’t know about hyperacusis. Otherwise, they might have warned me to be cautious during the test.
About 10 days later, I had a sound injury from someone calling me and their voice projecting into my right ear. I felt a severe sharp pain deep “in” the ear, and became very sensitive to ordinary noise. Looking back, I believe I was already becoming sound sensitive because I had been at a weekend event where there was a lot of noise and door slamming. I’ve often wondered whether some extensive dental work a few months earlier might have been a causative or contributing factor, too.
Timeline:
- January 2008: Definite onset of hyperacusis.
- April 2008: First set of audiograms with LDLs. Tried Neuromonics and then sound generators, but couldn’t tolerate either due to reactive tinnitus and ear pain.
- May 2008: 1st LLLT consisting of 10 sessions over two weeks with a neurological chiropractor who used LLLT for a variety of neurologic conditions. Definite subjective improvement though did not have follow-up LDLs done.
- October 2008: Tried sound therapy a second time from a highly experienced audiologist but had to quit after 6 weeks due to severe ear pain with even a few minutes of sound at the lowest setting. I understand others may have better results but in my case the pain from this particular treatment took many months to fade.
- January 2009 through September, 2015 – Irregular but noticeable improvement in tolerance for environmental sounds but socially isolated especially because of intolerance to certain qualities of sounds (staccato, motors, electrical equipment, tearing paper or tape, high-pitched voices).
- September – October 2015: Second course of LLLT in 14 sessions over five weeks at Otoclinica in Madrid and Barcelona. Very definite subjective improvement as well as LDLs, though still bothered by certain sound qualities as above (though less so).
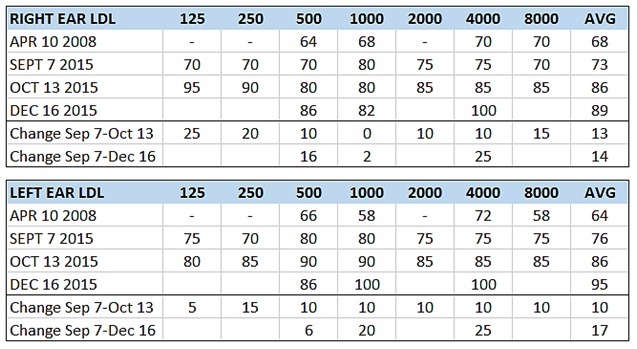
Below are my LDLs from 4 tests: (1) April 2008 (pre-LLLT first series from an audiologist who treats tinnitus and hyperacusis); (2) Sep. 7, 2015 (just before LLLT second series); (3) Oct. 13, 2015 (just after LLLT second series); and (4) Dec. 16, 2015 (from same audiologist as April 2008). LDLs reported as “100+” mean above 100 but not testable by the equipment. All audiograms showed mild high frequency hearing loss, an indicator of noise-induced hearing loss. AVG means simple averages, which may not be entirely scientific.
Below are simple averages of my LDLs over time. Note that audiograms one and four have fewer LDL readings, and that the horizontal axis is not to scale.
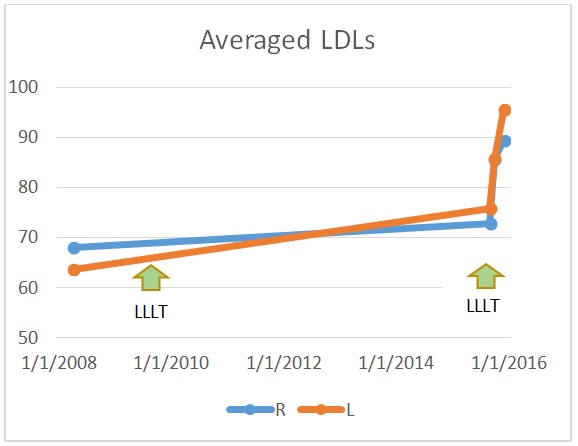
Equal-periods X-axis chart
My experience: After LLLT series one, I was better able to tolerate general street noise, delivery trucks and normal conversation; but sounds with “rough timbre” like power tools, crinkling bags, tearing paper and hammering caused reactive tinnitus and/or pain. My frequency of setbacks diminished significantly. I felt I had plateaued by 2009 and still avoided most social gatherings where music was playing. I often wore sound protection when walking in the city. I had gained about 10 decibel LDL improvement up to this point in time.
After LLLT series two, I could tolerate general sounds even better and could attend some social events with no, little or moderate protection. I had to wear some ear protection when going out in Madrid and Barcelona, where there was a lot of construction during my visit. Reactive tinnitus and hyperacusis seem to resolve more quickly, but rough timbre or certain voices still bother me even when well below my LDLs. Still, I can tolerate being in environments where before LLLT I had to wear earmuffs.
I do not get ear pain as quickly, and when I do it goes away faster. In general, life is easier, more comfortable and more available to me. So I believe that LLLT has made a major difference for me, but I still have a way to go. The doctors in the US and Spain used different approaches, but both looked not only at my ears but also at my overall state of physical wellbeing. Since I don’t have details on their protocols, I can’t compare them.
Taken by themselves, my LDLs say I now have mild hyperacusis. But that’s not yet my experience. LDLs test my response to pure tones in a non-fatigued state. Clearly they are measuring something important, but what?
Because many sounds still remain too uncomfortable for me (like high-pitched voices, power tools, ripping tape), it is unclear what mechanism LLLT is impacting. Do we need to better characterize hyperacusis with dimensions that may more precisely reflect the full functionality of the auditory system, such as: Sound-fatigue (reduced tolerance as the day goes on or when tired); sound timbral quality (discomfort leading to pain or tinnitus far below the pure-tone LDL); presence of pain; presence of reactive tinnitus?
Whether LLLT “works” and who’s best suited to it is a matter of scientific inquiry. But are we asking the right questions about how to characterize and evaluate hyperacusis and the other symptoms of noise injury?
In my personal experience, LLLT was very helpful. I would be happy to increase my LDLs, of course, but also need improvement in my tolerance for certain sounds that are well below my LDLs. Perhaps more LLLT will provide additional improvement. Perhaps I have a degree of irreversible cochlear damage that LLLT cannot affect. Perhaps something in the higher levels of the auditory brain centers are affected. Certainly we—as a community—can benefit from being more curious and scientific, and from developing measures that reflect the important components of our experience.
Would I recommend LLLT for someone with hyperacusis? My intent is to tell my story with the goal of promoting a better understanding of hyperacusis and to send the message that LLLT deserves to be researched. Speaking for myself, it has helped substantially, especially with LDLs and to some extent with my ability to be out in the world. Compared with many other medical treatments, its cost is reasonable (though anyone with hyperacusis may have to consider the cost of travel and ability to travel). If you’re considering it, find someone who knows what they’re doing! Protocols and precise “aim” of the tool are very important.
[i] While no prospective randomized or retrospective controlled studies of LLLT have been published to date, two large case series have been. (1) Zazzio M. Pain threshold improvement for chronic hyperacusis patients in a prospective clinical study. Photomedicine and Laser Surgery 2010;28(3):371-377; and (2) Prosper J, Graffelman J. The analysis of audiometric measurements before and after low-level laser therapy of Spanish patients with hyperacusis. (Published as a white paper – no journal given). Publication of an abstract: Prosper J, Hack E. Hyperacusis and other inner ear disorders are improving after light irradiation with photobiostimulation laser. Otolaryngology Head & Neck Surgery 2014;151(1 suppl):P208. Both reported favorable results. Zazzio’s study used LLLT, a pulsed electromagnetic field generator and antioxidants; and the performance of control arms of published tinnitus studies as the comparison (no-LLLT) group. Prosper’s study used only LLLT and patients served as their own controls.
Check out Dr. Wilden’s site on the web. German doctor. I have made good progress using his portable low level laser machine.
Hi Sandy, for how long have you been using the portable machine? Does it worth it?
Hi sandy is that dr you saw located in the US?! I’ve been having hearing loss and tinnitus for 2 years now. It kills me every day
Hi, i have question for author of this article. Can u be more specific about your lllt therapy,first in US and second in Spain, did you use ONE laser beam directly to ear cannal, or MORE (3 or 4) laser beams pointed from distance to ear cannal and surounding places?
Why u didn’t approve my question?
I wouldn’t trust anything that comes out of Otoclinica. The guy in that franchise (!!!) J Prosper tried to fudge the before and after of my LDLs to prove improvement and tried to diagnose me with misophonia when I pointed out his funny business to abstain from any responsibility for lack of improvement. If you ever wonder how he gets such high improvement stats (90 or 95 per cent) for hyperacusis on his ‘whitepapers’ it’s because he promptly shifts the goal posts like he did with me when things go south. I went on to look into it and realised that I could have hyperacusis or myoclonus, nobody knows, least of all him, but misophonia no way. Misophonia anyways is bs peddled by lazy Jastreboffian fanbois, especially if applied to me and the vibrations inside my ear. Prosper’s research is of course terrible because he’s just a middleman translator like so many in Spain. He has terrible research claiming improvement with tinnitool with a sample of one patient on a big poster on his office, when even Wilden has had to try to cover his past association with 5mw lasers. He doesn’t seem to care to make the difference between vestibular hyperacusis with dizziness or a stapes that seems out of place like Silverstein would, in case that means all he’s curing is herpes. The laser he uses is discussed over at tinnitustalk and can be bought entirely from China for the price of those 15 or 20 sessions, maybe even cheaper according to some newer threads in the forum I dunno. Another local doctor told me he or one of his associates are trying to act as middlemen with the laser business by visiting local ENTs, but their research is beyond crap, all the worse when Prosper publishes audiometric improvements irrelevant to LDLs or when Zazzio was called out when he claimed lack of conflict of interest in one his papers.
What is it exactly that LLLT is supposed to do at the physiological level that makes it a possibility for treatment?
It isn’t completely clear but there are a few possibilities. The main one relates to reducing inflammation. If we find (as is suspected) that inflammation in the inner ear plays a role in the hyperacusis pain process then reducing that inflammation would be important. It is well established in other work (e.g. with joint issues) that LLLT can help reduce inflammation. These detailed ideas need funding to be researched.
I have long suspected that inflammation was probably present, and that would explain the “spike” principle fairly well. I suppose than the next question should be: why don’t steroids seem to work better than they do? The answer may lie in the volume/capacity of the regional blood supply that carries them to the site of inflammation, or the whether dose sizes that get used are enough to get the levels high enough where they are needed (which also probably relates to the first answer). Do you have any new experience/reports of steroid use in hyperacusis? Could hyperacusis be part of a chronic inflammatory process that doesn’t settle after the initial insult?
“Whether LLLT “works” and who’s best suited to it is a matter of scientific inquiry.”
Breath not being held.
There is a paper: Role of Low-Level Laser Therapy in Neurorehabilitation (2010) Hashimi et al. that compliments the Norena (2018) paper An Integrative Model Accounting for the Symptom Cluster Triggered by Acoustic Shock. If I read this correctly (both very technical), Norena indicates an “ATP-crisis” in the tensor tympani muscle, which sets off the cascade of inflamation, pH changes, and other neurochemical changes that seem to cause the burning, fluttering, stabbing pain, etc. Hashimi’s paper mentions LLLT as triggering an increase in ATP in the cellular level. So perhaps it is helping to short-circuit the cascade of symptoms? That’s what I’m thinking. And it helped my insurance accept the LLT treatment.
God bless Dr. sebi for his marvelous work in my life, I was diagnosed of HERPES since 2014 and I was taking my medications, I wasn’t satisfied i needed to get the HERPES out of my system, I searched about some possible cure for HERPES i saw a comment about Dr. sebi, how he cured HERPES DIABETES and CANCER with his herbal medicine, I contacted him and he guided me. I asked for solutions, he started the remedy for my health, he sent me the medicine through UPS SPEED POST. I took the medicine as prescribed by him and 14 days later i was cured from HERPES, Dr. sebi truly you are great, do you need his help also? Why don’t you contact him through [email protected]
Happiness is all i see now I never thought that I will be cured from HERPES virus again. I have been suffering from a deadly disease (HERPES) for the past 3 years now, I had spent a lot of money going from one places to another, from churches to churches, hospitals have been my home every day residence. Constant checks up have been my hobby not until this faithful day, I was searching through the internet, I saw a testimony on how DR Aba helped someone in curing his HERPES disease, quickly I copied his email which is [email protected] just to give him a test I spoke to him, he asked me to do some certain things which I did, he told me that he is going to provide the herbal cure to me, which he did, then he asked me to go for medical checkup after some days after using the herbal cure, .behold I was free from the deadly disease, he only asked me to post the testimony through the whole world, faithfully am doing it now, please brothers and sisters, he is great, I owe him in return. if you are having a similar problem just email him on ( [email protected] ) or you can whatsApp his mobile number on +2348107155060
Hi I did contact him he is in Nigeria. He said he can help me with my hyperacusis.my question is did you trust him to send money and get your medication?
April 10, 2017
My wife suffered a left hear hyperacusis injury at a gun range 12 weeks ago despite ear protection and we are desperate for some direction. We tried steroids with no relief. There is no pain involved and very little tinnitus, but she cannot be in almost any type of social situation. Today is the first day of my ‘research’ into various treatment possibilities. Is there any reason to not try LLLT or herbal supplements? There doesn’t seem to be much else in the way of treatment (unless I’m missing them in my reading). Can anyone direct us to treatment center(s)? We live in the Atlanta Ga area but will travel if need be.
Norman,
Have you considered seeing Dr Nagler, who is in Atlanta?
I have also been trying LLLT in the US. I noticed an improvement after six weeks of twice a week therapy. This included LLLT, eye movement exercises, and hand/eye coordination type exercises. The burning decreased, the variety of tinnitus sounds decreased as well as volume, overall sensitivity decreased some. But still got fatigued quickly when “focused-listening” and stress would exacerbate symptoms. I had to stop for 9 months, but am starting again, with a pre-LDL measurement and will do a post-LDL when my sessions run out. Hopefully I can see an improvement since I only have a small window (10-15 dB) of comfort above my severe hearing loss.
Sharon Matas I never believed i would be healed someday.This disease started circulate all over my body and i have been taking treatment from my doctor, few weeks ago i came on search on the internet if i could get any information concerning the prevention of this disease, on my search i saw a testimony of someone who has been healed from (Hepatitis B and Cancer) by this Man dr.okorom and she also gave the email address of this man and advise we should contact him for any sickness that he would be of help, so i wrote to [email protected] telling him about my (HERPES Virus) he told me not to worry that i was going to be cured!! hmm i never believed it,, well after all the procedures and remedy given to me by this man few weeks later i started experiencing changes all over me as the Doctor Shapson assured me that i have cured,after some time i went to my Dr to confirmed if i have be finally healed behold it was TRUE, So friends my advise is if you have such sickness or any other at all you can email dr.okorom on : [email protected] or call +2348158168556 http://dr-okorom.webs.com/
Dr. Peter healed me from HERPES. I am., from UK. I was diagnosed of Human
papillomavirus{HERPES} in the year 2012 ever since then i was taking my medications, until i contacted the great herbalist. I saw many testimonies on how a great Herbalist cured their different diseases. I decieded to contact him, I was having HERPES for 5 years, but Dr. Peter sent me herbal treatments that healed me. I am HERPES free now, i have a new husband and i am so excited. His herbal treatment works like a magic.
If you have,HIV, cancer, syphilis. diabetes, hepatitis B, Asthma, arthritis, Human papilloma virus (HERPES), Infertility or any illness. Dr. Peter can also heal you. His email: [email protected] or call +2348143044267. Good luck!
Here is my details also if you wish to contact me personal:::: [email protected]
Sharon Matas I never believed i would be healed someday.This disease started circulate all over my body and i have been taking treatment from my doctor, few weeks ago i came on search on the internet if i could get any information concerning the prevention of this disease, on my search i saw a testimony of someone who has been healed from (Hepatitis B and Cancer) by this Man dr.okorom and she also gave the email address of this man and advise we should contact him for any sickness that he would be of help, so i wrote to [email protected] telling him about my (HERPES Virus) he told me not to worry that i was going to be cured!! hmm i never believed it,, well after all the procedures and remedy given to me by this man few weeks later i started experiencing changes all over me as the Doctor Shapson assured me that i have cured,after some time i went to my Dr to confirmed if i have be finally healed behold it was TRUE, So friends my advise is if you have such sickness or any other at all you can email dr.okorom on : [email protected] or call +2348158168556 http://dr-okorom.webs.com,,
I never believed i would be healed someday.This disease started circulate all over my body and i have been taking treatment from my doctor, few weeks ago i came on search on the internet if i could get any information concerning the prevention of this disease, on my search i saw a testimony of someone who has been healed from (Hepatitis B and Cancer) by this Man dr.okorom and she also gave the email address of this man and advise we should contact him for any sickness that he would be of help, so i wrote to [email protected] telling him about my (HERPES Virus) he told me not to worry that i was going to be cured!! hmm i never believed it,, well after all the procedures and remedy given to me by this man few weeks later i started experiencing changes all over me as the Doctor Shapson assured me that i have cured,after some time i went to my Dr to confirmed if i have be finally healed behold it was TRUE, So friends my advise is if you have such sickness or any other at all you can email dr.okorom on : [email protected]
I found a DO who was very knowledgeable of the content of Nunez paper, and willing to work with me. He has worked with many patients suffering from concussion injuries and some have also had tinnitus and hyperacusis resulting from that. I saw him twice a week for two months, and noticed improvement. (small, but progressing) One of the treatments was LLLT, in addition to exercises that worked with the concept of brain plasticity, integrative neurology. I had to stop suddenly when my Workers Comp Board reversed their approval, and noticed within a week or two an increase in my sensitivity and tinnitus. We are appealing, so hopefully will return. I have to drive two hours each way, but I think it was worth it. I plan to use the above comment and research to help support my appeal.
The use of lasers for marking metals is typically used for marking products with their characteristics and codes for tractability. This kind of application is found in electronics and electrical industry, mechanical engineering and the tool manufacturing industry, in sheet metal processing, in medical technology, in promotional items, jewelry and in the automotive industry.
Karen Tinsley, I’m interested in knowing which LLLT clinic or doctor you saw. Having a hard time figuring out who’s experienced in treating hearing loss / tinnitus patients in America. And you insurance accepted it?! Sweet deal.
Even if I can’t get there now due to COVID, I would love to see who I could be seen by. Otherwise it’s home device treatment for me. I’m seeing enough to make me think it’s worth the try.
Megan
Looking for LLLT treatment in Texas or somewhere in the US for my wife’s hyperacusis. Its bad, stuck at home.