Dan Polley in his laboratory (all photos courtesy of Dan Polley).
We asked Dan Polley, one of our scientific advisors, about his auditory research. Dan is currently a professor of otolaryngology at Harvard Medical School and the Director of the Eaton-Peabody Laboratories at Massachusetts Eye and Ear, the world’s largest academic research center devoted to the study of hearing. Dan spoke at our fall fundraising dinner in Boston.
Dan’s research focuses on the connections between brain plasticity and the perception of sound, with a particular interest in how the brain’s plasticity can be leveraged to eliminate the experience of tinnitus and loudness hyperacusis. His own tinnitus constantly reminds him of this goal and motivates him and his lab to work as hard as they can to help people who experience more severe versions of tinnitus and hyperacusis.
_______
In conversation with Joyce Cohen
After the Boston Marathon bombings in 2013, hundreds of people at close range to the explosives suddenly acquired tinnitus. They needed research scientists to help develop software for testing and managing their tinnitus. My team volunteered to help. I get satisfaction in focusing my science on practical applications. Hearing disorders like hyperacusis and tinnitus fall between the cracks of modern medicine.
I hope that we will soon be able to offer meaningful care and management for these disorders. My personal goal is to be a champion for these disorders and to develop more effective therapies and provide some sort of relief for people who feel overly sensitive to the auditory world, whether they have loudness hyperacusis for sounds in the environment or tinnitus for sounds in their own head.
I am a neuroscientist. I study the brain. I am not an ear doctor but I work closely with dozens of ear doctors. So I think I understand the problem of hearing disorders both from the perspective of the ear, a sensory organ that converts sound waves into electrochemical signals, and from the perspective of the brain, which converts those electrochemical signals into our conscious experience of sound.
SOUND PROCESSING GONE OFF THE RAILS
Loudness hyperacusis and tinnitus are fundamentally different from hearing loss. They are typified by what people cannot stop hearing, rather than what cannot be heard. These disorders might be triggered by an insult to the ear – or more specifically, the nerve connecting the ear to the brain – but the experience of these disorders is rooted in sound processing that has gone off the rails in the brain.
Correcting the physical degeneration in the ear that may or may not have initially triggered the tinnitus and hyperacusis could – in theory – eliminate these disorders. But there is no compelling reason to believe ear-based treatments for these disorders are on the near horizon. The large biotech and pharmaceutical companies that develop drugs and genetic medicine for the inner ear would love to tackle tinnitus and sound sensitivity, but I am unaware that any of the major players have active research programs on these topics.
There are a few reasons why the large inner ear biology firms aren’t tackling tinnitus and hyperacusis in the clinical programs. One factor is that the typical ear of someone with tinnitus and loudness hyperacusis is older, with chronic damage and degeneration spread across multiple cell types. Most of these companies are targeting hearing protection or gene therapy for monogenic disorders in otherwise pristine ears. Tinnitus and hyperacusis are on the other side of the spectrum and, even though there is an obvious market for therapies in this area, the targets for those therapies in the ear are not clear.
Another factor is that there aren’t direct objective measures of tinnitus and loudness hyperacusis like there are for hearing loss. My colleague, Stéphane Maison, and I are working to develop a new class of direct measures for auditory nerve degeneration and the psychological burden of tinnitus and sound sensitivity disorders. We started working on these questions only a few years ago and our initial findings are quite promising. We hope that the measures we introduce will encourage the hearing health companies to take up these new measurements for their clinical assessments and start clinical trials.
But I’m certainly not going to wait for them. I think the road to more effective, less invasive, and faster developing treatments for tinnitus and loudness hyperacusis lies in focusing on the brain and not the ear.
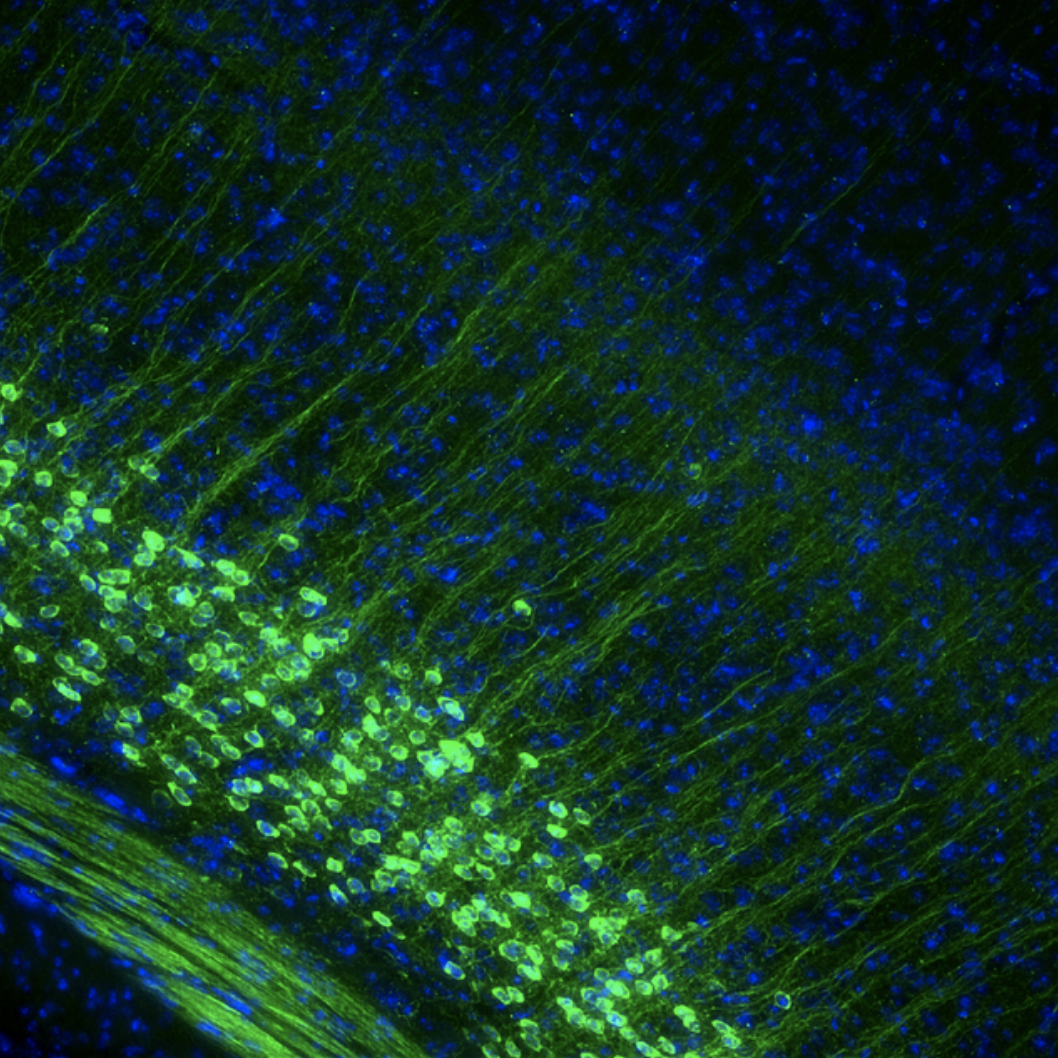
Neurons in sound processing centers of the neocortex are shown in green.
HYPERRESPONSIVITY TO SOUND SIGNALS
The underlying cause of tinnitus and loudness hyperacusis seems pretty clear, at least to me. Like your car, the brain has one network of nerve cells (neurons) that functions as the gas pedal and another that functions as the brakes. With auditory nerve damage, aging, or myriad other factors, the braking systems in sound-processing centers of the brain stop working well. Without normally functioning brakes, the “go” networks in sound-processing centers of the brain become hyperactive, their firing patterns become abnormally synchronized even when there aren’t audible sound signals in the environment, and they become massively hyperresponsive when sound signals are present, even when those sound signals are not especially intense.
This horrible triad of symptoms in sound processing centers of the brain – hyperactivity, hypersynchrony, and hyperresponsivity – is the cause of phantom sound perception and the reason why loudness becomes disproportionate to intensity. These symptoms are not, per se, an explanation for why some people are so bothered by their tinnitus, while most regard it as a mild nuisance. Nor are they the explanation for why sounds are merely perceived as too loud for some with loudness hyperacusis, while for others sounds are also experienced as intensely irritating and aversive.
To understand the immense psychological burden experienced by some people with tinnitus and loudness hyperacusis, one has to consider how the hyperactive, hypersynchronized, and hyperresponsive outputs from the sound processing centers of the brain disrupt brain systems that regulate emotional processing (which we call limbic networks), attention (which we call executive control networks), and arousal networks that regulate sleep states. The broader constellation of distress, aversion and lifestyle disruption that can accompany tinnitus and hyperacusis almost certainly depends on how and whether the abnormal activity patterns in sound processing centers of the brain have the knock-on effect of also disrupting the activity pattern in limbic, executive, and sleep networks of the brain.
This model for understanding the causes of tinnitus and loudness hyperacusis makes a few predictions, which we have tested in our laboratory. One prediction is that we can completely reverse loudness hyperacusis simply by reconnecting the braking systems in auditory centers of the brain. Recent studies in my lab show this to be true.
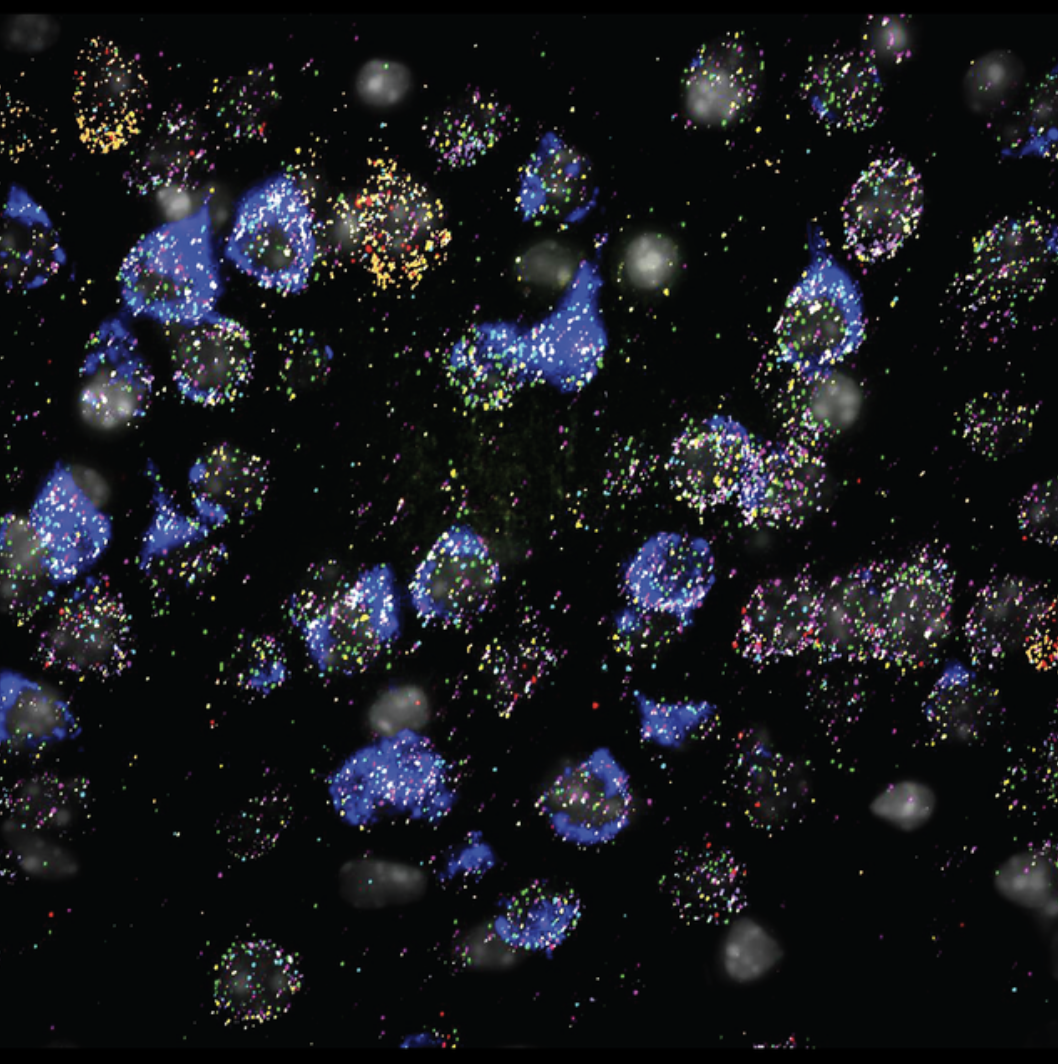
Bright dots show messenger RNA encoding different subunits of acetycholine receptors in sound processing centers of the neocortext.
AN INHIBITORY NEURON IN THE BRAIN
We have trained mice to behaviorally categorize a sound as soft or loud. After a restricted portion of the cochlea is damaged by intense noise, sounds that activate intact portions of the cochlea are perceived as louder than they used to be ( i.e., the mouse has loudness hyperacusis). Importantly, we can directly activate a type of “brake” neuron in the brain and the loudness hyperacusis immediately, although temporarily, disappears. Think about that: The mouse developed loudness hyperacusis after intense noise exposure but the hypersensitivity can be immediately taken away by increasing the activity of a type of inhibitory neuron in the brain, even though the ear remains damaged. This is the strongest evidence yet that the experience of loudness hyperacusis can be traced to abnormal activity patterns in the brain.
Further, hyperacusis was reversed by adjusting the brakes way downstream in the sound processing pathway. Even though there was abnormal activity in the cochlea and brainstem, we adjusted the activity of a cell type in the neocortex – where the conscious perception of the world is shaped – and the hyperacusis immediately went away. We have been fiddling with various ways to “pump the brakes” in these cortical inhibitory neurons and have found a few strategies that rely on just 15 minutes of direct inhibitory activation to produce more than a week of hyperacusis reversal.
The approaches we use are designed only for laboratory research but we think they could point us toward non-invasive approaches that could be used in humans down the road. We use a technique called “optogenetics” to precisely control the firing patterns of genetically distinct types of neurons with lasers. One approach involves pulsing the laser so that a particular type of “brake” neuron is activated at 40 Hz and entrains the entire cortical network to fire in an intense and sustained gamma rhythm. Another approach involves using optogenetics to simultaneously activate that same kind of brake neuron while also activating cholinergic basal forebrain neurons, which can be thought of as regulators of plasticity in adult brains.
OBJECTIVE MEASURES IN EYES AND FACE
Another prediction of the model above is that the difference for people who are mildly bothered versus those who are massively debilitated by their tinnitus and sound sensitivity can be found in how sound engages limbic brain systems that regulate emotional processing. Another study that is now in review for publication has identified objective measurable signals that predict the psychological burden of sound sensitivity and tinnitus.
This is an important breakthrough and it came by breaking with tradition, and looking for roots of tinnitus and sound sensitivity disorder in the eyes and face instead of focusing on the ear and sound processing centers of the brain.
To find measures that tracked the distress and aversion people reported, we focused our attention on aspects of human biology that have not really been studied in this context – the pupils and face. There are hidden signatures of tinnitus and sound sensitivity distress in the pupil and facial movement dynamics that are far more accurate than any of the purely auditory measures we have studied.
Emotionally evocative sounds elicit pupil dilations and subtle movements of the face. In persons with debilitating tinnitus and sound sensitivity, we found that the pupil dilations and facial movements were reliable and accurate “tells” (to borrow a term from poker) for their level of psychological distress. These measures provide us with automatic and objective markers for their disorder. With these markers in hand, we can use them to assess the efficacy of treatments and even stratify tinnitus and hyperacusis into different subtypes based on data instead of on intuition or superficial phenomenological qualities.
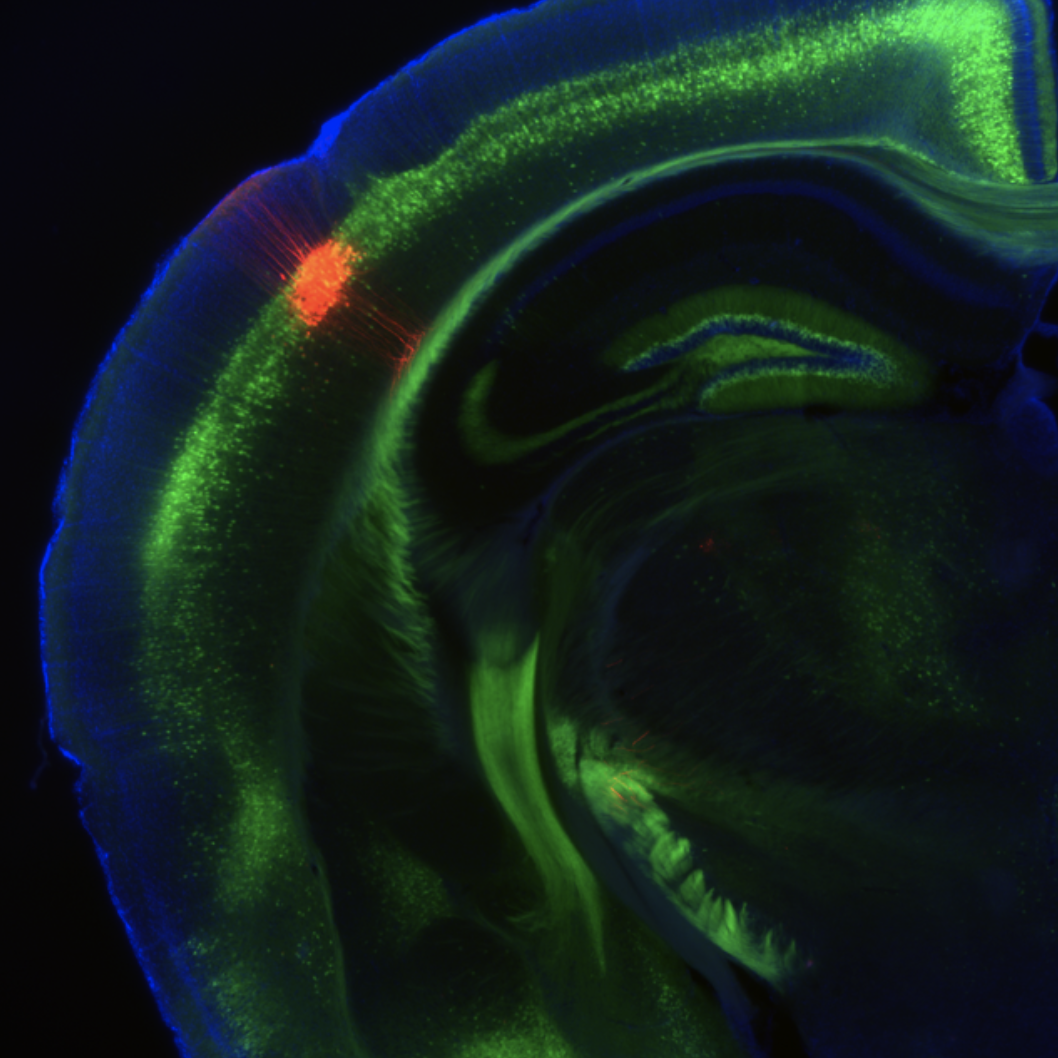
Neurons in sound processing centers of the neocortex, shown in red, connect with the striatum, a brain structure that coordinates sensory inputs and motor outputs.
A LONG WAY TRAVELED, BUT STILL FAR TO GO
Findings like these are paving the way toward a future where we understand the causes of tinnitus and hyperacusis and have useful treatments that will allow people to reengage with the auditory world. Studies in laboratory animals and studies on biomarkers are useful and important but more of the top researchers in our field need to come down from their ivory towers and get their hands dirty working on treatments for the people who need them the most. Looking ahead, this will be my main focus. I want to develop effective treatments and we are going to find them with the courageous members of the community who have tinnitus and sound sensitivity and are willing to partner with us to find the future treatments.
There is a long way to go and we don’t have enough funding or talented scientists working on these important problems. Also, you’ll notice that I have avoided saying anything about hyperacusis with pain. I’ll be the first to admit that I don’t understand the pain component that sometimes appears with hyperacusis. I wish I did but the intense subjective experience of pain isn’t something that my particular scientific toolbox allows me to understand.
My motivation for devoting my professional career toward these conditions comes from people who wrestle with their hearing disorder and who strive to maintain their identities in their home and workplace in spite of their personal torment. In my lab, we have a quote from Beethoven framed on the wall, “But that jealous demon, my wretched health, has put a nasty spoke in my wheel… for the last three years my hearing has become weaker and weaker. My ears continue to hum and buzz day and night. Sometimes I can scarcely hear a person who speaks softly… but if anyone shouts I can’t bear it. Heaven alone knows what is to become of me.” This quote speaks to hearing loss, tinnitus, and loudness hyperacusis not as compartmentalized hearing disorders but as whole life disorders.
Beethoven wrote that in a letter to a friend in 1801. We have come a long way in the last 223 years, even for the relatively ignored medical conditions that relate to hearing disorders. There are five active clinical trials showing that children born with a mutation that causes profound hearing loss can be cured with genetic medicine delivered to the cochlea. There have been five publications showing meaningful reductions in tinnitus severity through combined auditory and tactile stimulation. When it comes to tinnitus and hyperacusis, we are just at the beginning of developing meaningful therapies. But we have a foothold on the mountain to reach low-cost, effective, and widely available treatments. Now, what we must do is climb.
Still no where near. Not in most of our lifetime
Thank you Dr. Polley for your research and this insightful article.
You mention that there is currently no objective measure of tinnitus. This has actually been achieved a few years ago: https://www.sciencedirect.com/science/article/pii/S0378595522000600
Hyperacusis Central has interviewed one of the researchers behind this method (https://hyperacusiscentral.org/detecting-tinnitus-in-the-brain-an-interview-with-emilie-cardon-phd/), and made a video summary of the interview (https://www.youtube.com/watch?v=9b3s_vozNAA).
I applaud Dr Polley’s brilliant and insightful article for our newsletter. His work as well as other researcher scientists are truly inspirational. He gives my son and many other sufferers hope. I remain confidant that we will have effective treatments within the next several years if not earlier.
Hi Dr. Barad – what can realistically be done to re-purpose current pharmaceutical drugs for off label hyperacusis treatment or initiate studies that aim to investigate drugs to mute this over-reactivity and central processing? Why do neurologists and ENTs insist on a revolving door where they pawn patients off on the other specialty?
Thank you Dan for such a clear description of the work you and your team is doing.
Interesting article and very important research. Thanks for that!!
What about laser therapy on the brain?
Eternal gratitude to Dan Polley for his research. Thanks to him and Stéphane Maison, we can see the light at the end of the tunnel. Thank you for sharing these scientific advances with us. Having a foot on this mountain is already beautiful, and we sincerely hope one day to see the flag of salvation there… THANK YOU!
In like 2 decades maybe
👍♥️👍
”I’ll be the first to admit that I don’t understand the pain component that sometimes appears with hyperacusis. I wish I did but the intense subjective experience of pain isn’t something that my particular scientific toolbox allows me to understand.”
An article for Dan then:
https://hearinghealthfoundation.org/blogs/understanding-pain-signals-triggered-by-damage-to-the-inner-ear
As always, everything will be “sometime and somewhere.” Every day is torment for such patients, and there is no treatment.
I wish they would hurry up. Sounds like they understand what is happening so get the treatment sorted.
Excellent article, Dan. Very encouraging.
Have you ever researched a connection between hyperacusis/tinnitus & atlas subluxation? This journey began for me after whiplash/tbi sustained from a car accident. The only temporary breaks I’ve experienced since have been after NUCCA treatments. Curious…
For a number of years i have had a a whoshing sound in my head sometimes very loud all i get from ENT is it a problem with my hearing. also local GP say it’sc a hearing problem. Now it has changed to a very loud roaring type whooshing noise.all the time day and night
I have no real or major problems hearing regardless of what they say
This article is insightful and encouraging. I had severe pain hyperacusis from a neck trauma. I rewired my own brain using the principles of Neuroplasticity and now my hearing is normal!!! For those reading this suffering from Hyperacusis, you can heal it! I consulted with Myriam Wescott (out of Australia) and she gave me strategies for healing. Ultimately, it is entirely individual though. It takes time, effort, and belief.
Thanks for the article! But as always, something may happen sometime later… And life goes away, it is impossible to live like this, having reactive tinnitus and hyperacusis of loudness..